Ιn recent years, magnetic resonance imaging (MRI) has transformed the prostate cancer (PCa) diagnostic pathway, based on the evidence of multiple high-level evidence studies (refs 4M, MRI first, and PROMIS). Taken together, the evidence indicates that prostate MRI before biopsy can allow one-third of men to avoid an immediate biopsy, reduce overdiagnoses and overtreatment of clinically indolent PCa, and detect at least as much clinically significant PCa (csPCa) as compared to a non-imaging pathway with random biopsies. If a suspicious lesion is found on MRI, the subsequent biopsy can be targeted.
Jasper Twilt, Radboud University Medical Center, Nijmegen (NL) and Maarten de Rooij, Radboud University Medical Center, Nijmegen (NL)
In the EAU Guidelines, MRI now plays an upfront role in an MRI-directed diagnostic pathway prior to prostate biopsies (ref: EAU Guideline). The Prostate Imaging Reporting and Data System (PI-RADS), initially introduced in 2012 and further refined to the latest iteration in 2019 (version 2.1), has standardised the reporting of prostate MRI and outlines minimal technical requirements for its acquisition (ref PIRADSv2.1). The scoring system, using a 1-to-5 score to describe the likelihood of the presence of csPCa enhances interdisciplinary communication with referring clinicians. Many years of deployment have led to a worldwide adoption and recognition of PI-RADS amongst the radiological and urological communities. Despite these efforts of standardisation, challenges persist.
In this article, these challenges are briefly discussed, together with the role artificial intelligence (AI) might play as potential solution.
Challenges of the MRI-directed prostate cancer pathway
Multiple studies evaluating PI-RADS consistently demonstrate high sensitivity and negative predictive values, indicating its ability to rule-out csPCa. However, it exhibits variable specificity and positive predictive values, leading to discrepancies among radiologists in the ability to rule-in csPCa, which in turn results in unnecessary biopsies.
A contributing factor to these variable results and high inter-reader variability is the level of expertise required for interpreting prostate MRI. The importance of education for radiologists (and radiographers) is underscored in a list of joint recommendations by the European Society of Urogenital Radiologists (ESUR) and the European Association of Urology Section of Urological Imaging (ESUI). These recommendations address the need of image quality assurance and control. Also, the minimum number of cases to be read before unsupervised reporting and to be considered as a basic or expert prostate radiologist are defined.
Beyond these technical and reporting challenges, there is a substantial increase in the number of men undergoing prostate MRI due to its prominent role in guidelines and adoption of prostate MRI in active surveillance and population screening. This increased workload can have negative effects on the image quality and diagnostic accuracy in a healthcare setting that is already facing the dilemmas of an aging population and personnel shortages.
Artificial intelligence
Artificial intelligence (AI) is a rapidly advancing field that has gained considerable interest in medical imaging research, particularly in preclinical settings. AI might be able to address (a part of) the aforementioned limitations within the PCa pathway and healthcare as a whole. AI includes various subsets of learning methods and algorithms.
Machine Learning (ML), a subset of AI, consists of algorithms that can learn and predict specific tasks without explicit programming. ML algorithms learn and predict by extracting and using features. In prostate MRI, these features are mainly derived from axial T2-weighted sequences and diffusion weighted imaging (DWI), potentially combined with clinical parameters like serum prostate-specific antigen (PSA) and PSA density.
More recently, a specific subset of ML, known as deep learning (DL), has gained popularity. In contrast to traditional ML, DL does not require prior feature extraction; instead, it learns to extract complex features during training. DL includes one dimensional feature input algorithms and convolutional neural networks (CNNs) using two- and three-dimensional feature input, as seen in prostate MRI. CNNs are commonly used in medical image analysis. Although DL does not need prior feature selection, it requires extensive training data.
Recent initiatives have greatly contributed to collecting and sharing of multi-centre prostate MRI data, attributing to increased performances of DL algorithms in general (ref: ProCAncer-I). However, the complex architecture of DL algorithms makes them less transparent and more challenging to interpret.
Role of AI in the diagnostic PCa pathway
Image interpretation
The most obvious role for AI lies in the image interpretation phase of the PCa diagnostic pathway. This is the focus of many prostate AI studies in current literature.
Numerous studies are performed to classify pre-annotated lesions into insignificant versus significant cancer and benign versus malignant lesions (ref Twilt review). Also, more advanced algorithms are aimed at automated detection and classification of PCa lesions. Performance of such algorithms have already achieved diagnostic accuracies on par with radiologists. However, while sensitivity values are often similarly good, most AI algorithms have difficulties in reducing the number of false positive findings (ref). Furthermore, most studies concern small cohorts, often without external validation, and have not been validated prospectively in a clinical workflow.
One of the prerequisites for a good AI algorithm is that it can help the radiologist in working faster or more accurate. Therefore, AI research should emphasise and evaluate the interaction between AI algorithms and radiologists, particularly in (simulated) clinical environments.
Recent studies have increasingly explored concurrent reading scenarios, wherein radiologists are assisted by AI-generated detections and diagnosis of PCa. Some studies have reported on improvement in diagnostic accuracy (ref: https://doi.org/10.1097/rli.0000000000000780 & https://doi.org/10.1148/radiol.222276), yet improper implementation of such techniques can prolong reading times and disrupt workflow, (ref: https://doi.org/10.1016/j.ejrad.2023.111252), highlighting the need to further investigate optimal implementation strategies.
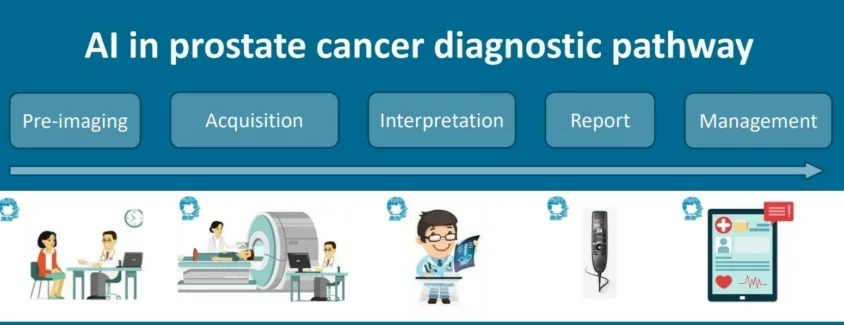
AI not only has the potential to enhance the detection of csPCa, but can also contribute to various other steps in the PCa diagnostic pathway, from image acquisition to patient management (see figure above).
Acquisition
Several studies have investigated the use of AI to speed up acquisition times of prostate MR images to potentially relieve capacity problems. These solutions often employ undersampling techniques alongside reconstruction methods, integrating AI for tasks such as denoising of images, artifact correction, and, notably in the case of DWI, synthesizing b-value images. While reducing acquisition times for prostate MRI is achievable, it is imperative to assess the preservation of diagnostic quality, particularly through prospective studies (ref: https://doi.org/10.1002/jmri.2…). Furthermore, lack of proper training data might lead to false pathologies being “hallucinated” in the reconstructed image (ref: https://doi.org/10.1073/pnas.1907377117). Still, promising results have been achieved in other fields within radiology, such as in musculoskeletal radiology.
A prospective study showed that knee MR images could be obtained nearly twice as quickly as with conventional acquisition techniques, while preserving comparable or even superior image quality (ref [https://doi.org/10.1148/radiol…).
Image-quality
Image-quality assurance and quality control are other potential applications of AI. Image quality is essential, because it can influence the next steps in an MRI-based diagnostic pathway, such as MR-targeted biopsies, risk stratification, and treatment decisions.
Decreased image quality is associated with increased rates of indeterminate (PI-RADS 3) findings. The
ESUR/ESUI recommendations also state that radiologists should assess the image quality of each prostate MR examination and mention this in the report. To enable this, a standardised approach for the assessment of image quality; the
Prostate-Imaging Quality (PI-QUAL) scoring system is available to evaluate image quality of a prostate MRI (ref PIQUAL).
In the future, automated methods based on DL have the potential to provide a more objective assessment of image quality. A few studies already demonstrated the capability of AI to independently detect suboptimal quality in prostate MRI imaging (ref: https://doi.org/10.1016/j.ejra…, while also suggesting a correlation between higher quality examinations and improved detection performance of csPCa (ref: https://doi.org/10.1002/jmri.2….
Other AI applications
Other AI applications that are of interest are the ones that enable automated detection of ‘normal’ or obvious frequently appearing conditions such as BPH or prostatitis. In breast imaging, studies have shown promising results in using AI to improve mammography screening accuracy while reducing screen-reading workload (ref: https://doi. org/10.1016/S1470-2045(23)00298-X). Additionally, scenarios where AI serves as a “first reader” to triage non-disease examinations have shown promising outcomes, boosting accuracy while reducing workload (ref: https://doi.org/10.1016/S2589) with high certainty. Moreover, AI acting as a “second reader” could potentially improve the responsiveness of radiologists, which is of particular interest to less experienced radiologists.
Future
Future applications of AI may, based on the combination of different (non-imaging) biomarkers, provide a prediction about which patients will benefit the most from imaging. AI could also predict which patients have a high chance to develop extracapsular extension, recurrence, and/or metastases, and thus it could allow for a more personalised treatment.
Furthermore, given the continued rapid advancements in technology and ongoing drive to share and create large multi-institutional datasets in the AI domain, it is anticipated that the capability of AI continues to expand. It is important that developers gain access to data and receive support in proper validation of their algorithms, with the involvement of clinical experts. The PI-CAI challenge serves as an exemplar of such an endeavour, where AI developers were granted access to public data and resources to retrain and validate their algorithms in a transparent and fair manner, while also undergoing benchmarking against a large cohort of radiologists (ref: https://pi-cai.grand-challenge…).
Limitations
AI is often deployed as an aid on a specific sub-task of the radiologists work, with data from retrospective controlled reader-environments. It is imperative that implementation studies involving AI are initiated to truly assess its added value in clinical practice. An AI tool should primarily aim to streamline work processes and ideally alleviate burdensome tasks.
However, the introduction of such AI raises new questions: Who is responsible for the outcomes of AI algorithms? How can we guarantee and control ongoing quality of AI as it encounters new prospective data? And who will finance the implementation of AI software?
Conclusions
To summarise, the expected rise in the number of prostate MRIs and the challenges that are accompanied with the current MRI-based diagnostic pathway of PCa, requires smart solutions. In most of these solutions, AI can play an important role. AI applications have the potential to improve the diagnostic quality of the prostate-MRI pathway and speed up the workflow. However, clinical validation of these tools is needed before fully exploiting their potential.
This article first appeared in the 2024 Congress News edition of the European Urology Today.